
689 views
Amal Johnson et al.: The Rubbish Rib Tickler – Successful Complete Surgical Removal of Large Symptomatic Rib Tumour
Case Report
The Rubbish Rib Tickler – Successful Complete Surgical Removal of Large Symptomatic Rib Tumour
Ajay Narasimhan1, Amal Johnson2 and Narasimhan.R3
1 Cardiothoracic Surgeon, Rajiv Gandhi Government General Hospital, Madras Medical College, Chennai, Tamil Nadu, India
2 Post graduate, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai, India
3 Senior Consultant, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai, India
ABSTRACT
Fibrous Dysplasia is a non inherited skeletal developmental abnormality, where normal bone is replaced by fibrous tissue and poorly formed area of immature bone. Monostotic lesions are 80% of the cases; and Polyostotic lesions are characteristic component of specific syndromes. It is usually detected in 1st and 2nd decade of life as an incidental finding and can cause occasionally dull aching pain2. The clinical course is variable and depends upon the extent and location of the lesion. Fibrous Dysplasia is the most common benign rib lesion3,4. In this case report, we describe a patient with large progressively increasing in size symptomatic rib tumour diagnosed as benign lesion with biopsy and underwent successful resection surgery.
Keywords: Fibrous dysplasia, bone, lesion, rib
Corresponding Author: Dr. Ajay Narasimhan M.Ch, Assistant Professor, Institute of Cardiothoracic Surgery, Rajiv Gandhi Govt. General Hospital, Madras Medical College, EVR Periyar Salai, Chennai – 600003. Ph : +91 9940137747.
Introduction
Fibrous Dysplasia (FD) is a non inherited skeletal developmental abnormality where normal bone is replaced by fibrous tissue and poorly formed area of immature bone1. The pathogenesis of the tumour is attributed to the activating mutation of the Gsa subunit of G protein coupled receptor, resulting in upregulation of cAMP2,3. Monostotic lesions are 80% of the cases; common sites of involvement are ribs, long bones, pelvis and skull4. Polyostotic lesions are characteristic component of specific syndromes, McCune Albright Syndrome (café au Lait spots and endocrinopathy causing precocious puberty) and Mazabraud disease (renal phosphate wasting and soft tissue myxoma)5,6. It is usually detected in 1stand 2nddecade of life as an asymptomatic,incidental finding and can cause occasionally dull aching pain due to external compression or fracture (fatigue/pathological). The clinical course is variable and depends upon the extent and location of the lesion. Polyostotic FD develop severe skeletal deformities by adolescence. FD is the most common benign rib lesion(6-20%)7,8. In this case report, we describe a patient with large symptomatic rib tumour diagnosed as benign lesion with biopsy and underwent successful resection surgery.
Case Report
A 61 year old gentleman a known diabetic/hypothyroid/Rheumatic heart disease Controlled AF/ – on regular medication came as an outpatient with complaints of right sided chest swelling present for more than 5 years- progressively increasing in size and right sided chest pain for more than 6 months(insidious in onset, dull in nature, associated with occasional breathing difficulty and dry cough, radiating to shoulder and back, aggrevated by movements and relieved by rest). No history of fever/weight loss. Patient had been evaluated by an orthopedician 5 years back –biopsy done under LA reported as Giant cell rich tumour and patient opted for conservative management back then. General examination – patient was not dyspneic with Spo2- 98% on room air, no pallor, no clubbing , no lymphadenopathy and no pedal edema. Local examination – patient had right sided swelling in anterior chest near the 2 nd rib area – 2 x 2 cm, hard, non tender with normal overlying skin. Chest Xray PA view showed a non homogenous, oval shaped right upper zone mass(Figure 1) . CT chest with contrast showed an expansile lytic destructive lesion involving the anterior end of the right 2 nd rib measuring 7.3cm x 5cm x 7.7 cm(Figure 2) with majority of lesion being intrathoracic.
Multidisciplinary specialist team (consisting of pulmonologist, orthopedician, pathologist, oncologist and thoracic surgeon) consensus was operative management and removal of tumour. Careful pre operative assessment done with clearance from cardiologist. Under GA, the tumour was removed in toto with segmental resection of 2 nd rib by cardiothoracic surgeon (Figure 5,6). Post operative uneventful and patient was discharged on 3 rd day post surgery with oral analgesics. HPE of tumour: Bone with intertrabecular marrow in foci and in other areas the expanded bone is being replaced by a lesion composed of irregular bony spicules with irregular cement lines and no osteoblastic rimming against a spindle cell stroma with scattered hemosiderophages focally. Some stromal hydropic and myxoid change is noted with separation of the spindle. Final Impression – Fibrous dysplasia(Figure 4). Patient was symptom free and comfortable when followed up as outpatient after one month.
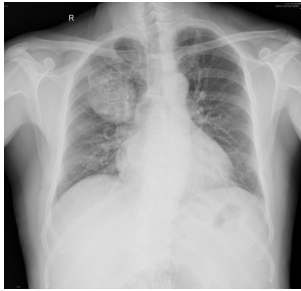
Figure 1

Figure 2
Figure 3
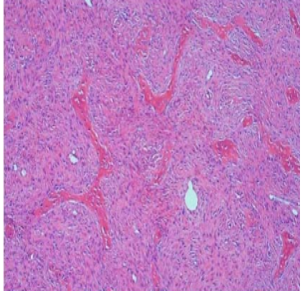
Figure 4

Figure 5
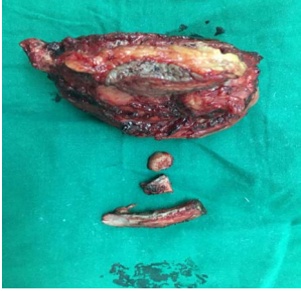
Figure 6
Discussion
Fibrous Dysplasia (originally described by Lichtenstein in 19386) is a benign bone disease characterized by the progressive replacement of normal bone elements by fibrous tissue and immature woven bone1. They represent 5-7% of benign bone tumours9,10. Monostotic fibrous dysplasia accounts for 80% of all cases4; the most common locations of involvement are the rib(6-20%), proximal femur, tibia, and skull. Polyostotic fibrous dysplasia accounts for the remaining 20% of cases and tends to involve larger segments of bone. It is also associated with more severe deformities and frequent fractures. Within the extremities,bowing and premature fusion of growth plates results in short stature. Shepherd’s crook deformity (coxa vara angulation of the proximal femur) and saber shin deformity (anterior bowing of the tibia) may also be seen. Fibrous dysplasia of the spine is associated with scoliosis11.
Radiographic features of fibrous dysplasia are variable. Classically, radiographs depict a wellcircumscribed lucent lesion in the metaphysis or diaphysis with a ground-glass appearance. The cortical bone may be thinned with diffuse endosteal scalloping. Periosteal reaction is usually not present unless it is associated with a pathologic fracture. Within a rib, fibrous dysplasia causes fusiform enlargement and may have a multiseptated appearance11. CT is the best technique for characterizing fibrous dysplasia. The sclerotic margin of the lesion is easily visualized and the cortical detail is superior to that of radiographs.Fibrous dysplasia enhances with administration of intravenous contrast material due to the inherent vascularity of the lesion12,13. MR imaging features of fibrous dysplasia are variable and depend on the amount and degree of fibrous tissue, cellularity, collagen, trabeculation, and cystic or hemorrhagic degeneration. The MR imaging appearance may not be helpful in differentiating fibrous dysplasia from other bone lesions. Signal intensity is typically low to intermediate on T1-weighted images and intermediate to high on T2-weighted images. Heterogeneous enhancement may also be present14.
Histologically, FD is characterized by progressive replacement of normal marrow and cancellous bone by immature bone and fibrous stroma. Histologically, trabeculae of immature bone are surrounded by a fibrous stroma of spindle-shaped cells without prominent osteoblastic rimming or malignant features. The trabeculae are dysplastic, non–stress oriented, and appear disorganized. This appearance has been likened to “alphabet soup”15.
The approach to chest wall swelling is history taking(duration, first symptom, associated symptoms like pain, progression, persistence, multiplicity, cause loss of body weight, surgery) and complete examination(inspection, palpation, press, percussion,auscultation, transillumination, surrounding tissue) followed by investigations(non invasive- CXR, CT/MRI; invasive- biopsy). The differential diagnosis of chest wall swelling include actinomycosis, sapho(synovitis, acne, pustulosis, hyperostosis and osteomyelitis) syndrome, teitze syndrome(costochondritis) and tumours(bone cyst, Fibroxanthoma , Giant cell tumour, lipoma, hemangioma, chondrosarcoma, neurofibroma,lymphangioma,metastases) and sebaceous cyst.7 The clinical course of fibrous dysplasia is variable and depends on the extent and location of the lesion or lesions. Less than 1% of fibrous dysplasia lesions undergo malignant degeneration to osteosarcoma (most common), fibrosarcoma, or chondrosarcoma. Patients may complain of increasing pain or development of a soft tissue mass. Radiographs may show new aggressive features such as periosteal reaction, cortical breakthrough, and areas of increased lucency7.
Treatment of monostotic fibrous dysplasia is dependent on symptom management and clinical presentation. Asymptomatic patients require no treatment, though follow-up radiographs every 6 months are recommended to ensure stability. Treatment with bisphosphonates may be used for pain relief in patients with polyostotic fibrous dysplasia . Symptomatic or atypical lesions may rarely require surgical excision for pain relief and for histologic confirmation8,16.
Conclusion
Fibrous dysplasia is a benign skeletal lesion that can involve one or more bones. Monostotic lesions are frequently observed incidently and most are asymptomatic. Polyostotic lesions are large and cause complications including pain, deformity and fractures along with skin lesions and endocrinopathy(McCune Albright Syndrome) and multiple myxomas(Mazabraud syndrome). Most monostotic lesions require only observation and operative treatment rarely in symptomatic lesions, atypical lesions, stabilize fracture and in correction of deformity.
Acknowledgement
We sincerely thank the management of Apollo Hospitals for their consistent support in our pursuit for excellence.
References
- Chapurlat RD, Meunier PJ. Fibrous dysplasia of bone. Baillieres Best Pract Res Clin Rheumatol. 2000;14:385–98.
- Weinstein LS, Shenker A, Gejman PV, Merino MJ,Friedman E, Spiegel AM. Activating mutations of the stimulating G protein in the McCune Albright syndrome. N Engl J Med. 1991;325:1688-95.
- Weinstein LS, Chen M, Liu J. Gs(alpha) mutations and imprinting defects in human disease. Ann NY Acad Sci. 2002;968:173-97.
- 6. Henry A. Monostotic fibrous dysplasia. J Bone Joint Surg Br. 1969;51:300–6
- 1. Lichtenstein L. Polyostotic fibrous dysplasia. Arch Surg. 1938;36:874-98.
- Lichtenstein L, Jaffe HL. Fibrous dysplasia of bone. A condition affecting one, several or many bones, the graver cases of which may present abnormal pigmentation of skin, premature sexual development, hyperthyroidism or still other extraskeletal abnormalities. Arch Pathol. 1942;33:777- 816.
- Kransdorf MJ, Moser RP Jr, Gilkey FW. Fibrous dysplasia.RadioGraphics 1990;10(3):519–537.
- Stanton RP, Ippolito E, Springfield D, Lindaman L,Wientroub S, Leet A. The surgical management of fibrous dysplasia of bone. Orphanet J Rare Dis 2012;7(suppl 1):S1




