
689 views
Amal Johnson et al.: Bronchoscopy quiz
Pictorial CME
Bronchoscopy quiz
Amal Johnson1 and Narasimhan.R 2
1Post graduate, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai
2Senior Consultant Pulmonologist, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai
Corresponding Author: Dr. Amal Johnson, Post graduate, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai
How to cite this article: Amal Johnson and Narasimhan.R, Bronchoscopy quiz, JAPT 2019:2(1):40-41
A case of Radio Bronchoscopic Dissociation
68 year old lady a known diabetic /coronary artery disease (on regular medication) came as an OP with complaints of cough with mucoid expectoration, wheezing and occasional breathlessness – present for the past 5 years which has worsened in the past 2 months. History of loss of weight (5kg in 3 months) without history of fever / hemoptysis / chestpain. No history suggestive of asthma. No past history of tuberculosis. She was treated with ICS/LABA by a local physician for past 5 years – no improvement.
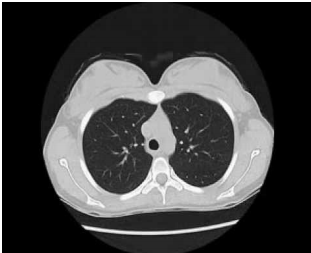
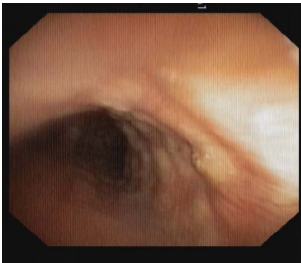
On examination, chest was clear and Spo2- 99% on room air. PFT was normal. Chest Xray did
not reveal any abnormality. CT chest showed mild narrowing of airways. For further evaluation, Bronchoscopy was done which revealed diffuse hard nodules in trachea and both bronchi with mucosal involvement, narrowing of lumen sparing the posterior membrane and mucous secretions seen bilaterally.
Access this article online
| Quick Response Code: | Website: www.aptchest.com |
What is this entity?
Answer:
Tracheobronchopathia Osteoplastica
Tracheobronchopathia osteoplastica is a benign chronic disease characterised by the presence of submucosal osteocartilageous nodules in the tracheobronchial tree (1,2). The reported incidence is 2-7 cases in 1000 bronchoscopies (3). It usually occurs in the sixth or seventh decade of life with a slight male predominance (1). The cause remains unknown and two theories postulated regarding the pathogenesis of the disease are 1) Virchows theory – nodule formation occurs due to the ossification and calcification of the ecchondromas (4). 2) Metaplastic theory – ossification of the elastic connective tissue (5). The predominant symptoms are chronic cough, dyspnea, wheezing, hemoptysis, recurrent respiratory tract infections (6).
The patients are often mistreated as asthma or chronic bronchitis. CT scan is the radiological investigation of choice which can pick up nodularity and calcification of trachea and bronchi in late stages (7,8). Bronchoscopy is the definitive investigation and usually biopsy is not required (9). There is no efinitive treatment and progressive disease causing airway stenosis requiring intervention occurs only in 15 % of patients(1,6).
REFERENCES
- Prakash UB. Tracheobronchopathia osteochondroplastica. Semin Respir Crit Care Med. 2002 Apr;23(2):167-75. PMID: 16088609.
- Chroneou A, Zias N, Gonzalez AV, Beamis JF Jr. Tracheobronchopathia osteochondroplastica. An underrecognized entity? Monaldi Arch Chest Dis. 2008 Jun;69(2):65-9. PMID: 18837419.
- Hussain K, Gilbert S. Tracheopathia osteochondroplastica. Clin Med Res. 2003 Jul;1(3):239-42. PMID: 15931314.
- Virchow R. In: Die krankhaften Geschwülste.1st ed (Vol. 1). Berlin; Hirschwald, 1863:442-3.
- Aschoff-Freiburg L. Ueber Tracheopathia Osteoplastica. Verh Dtsch Gesch Pathol. 1910;14:125-7.
- Jindal et al. Tracheobronchopathia Osteochondroplastica – A rare or an overlooked entity? Radiology Case. 2013 Mar; 7(3):16-25
- Marom EM, Goodman PC, McAdams HP. Diffuse abnormalities of the trachea and main bronchi. AJR. 2001 Mar;176(3):713-7.PMID: 11222211.
- Webb EM, Elicker BM, Webb WR. Using CT to diagnose nonneoplastic tracheal abnormalities: appearance of the tracheal wall. AJR. 2000 May;174(5):1315-21. PMID: 10789785.
- Prince JS, Duhamel DR, Levin DL, Harrell JH, Friedman PJ. Nonneoplastic lesions of the tracheobronchial wall: radiologic findings with bronchoscopic correlation. Radiographics. 2002 Oct;22:S215-30. PMID: 12376612





