
689 views
Selvi.C et al.: Prevalence of Anxiety and Depression in Stable Chronic Obstructive Pulmonary Disease Patients in a Tertiary Care Hospital
Original Article
Prevalence of Anxiety and Depression in Stable Chronic Obstructive Pulmonary Disease Patients in a Tertiary Care Hospital
Selvi.C1 and Narasimhan.R1
Department of Respiratory Medicine, Apollo Main Hospital, Chennai
ABSTRACT:
Introduction: Psychiatric disorders, especially anxiety and depression have been reported to have an increased prevalence in chronic obstructive pulmonary disease (COPD) patients, but there is a paucity of data from India. Aim & Objectives: To study the prevalence of depression and anxiety in stable chronic obstructive pulmonary disease patients presenting in a tertiary care hospital, To analyze the anxiety and depression in relation to level of airway obstruction as per GOLD criteria in chronic obstructive pulmonary disease patients. Materials and Methods: Patients present with a well-established diagnosis of COPD according to GOLD were included. In pulmonary function testing, a post-bronchodilator FEV1/FVC ratio of 8 indicates depression or anxiety. Results: Prevalence of anxiety in our study population of about 51.2% and prevalence of depression 56.2%. Prevalence of both anxiety and depression found in 37.5%. Males have more anxiety and depression which is statistically significant (for anxiety P=0.024,for depression P=.001) .Smokers have more anxiety and depression which is statistically significant(For anxiety P= .003,for depression P= .001) . Ex smokers have more anxiety and depression compared to current smokers(For anxiety P=.011,for depression p=.002). Anxiety and depression was not significantly associated with level airflow obstruction. (P value for anxiety .266).(P value for depression .299).Severity of anxiety and depression also not significantly associated with severity of airflow obstruction. Anxiety and depression was found to be increased if more previous exacerbation which is statistically significant(For anxiety P= .007,for depression p= .015).Depression was increased significantly if disease duration increases which is statistically significant(P=.001.Anxiety was found in68.3%urban population,31.7%rural population. Depression was found in 68.9%urban population, 31.1% rural population.
Conclusions: Anxiety and Depressive symptoms are common in all stages of COPD and the prevalence of anxiety depression in Indian patients with COPD is high. Patients with COPD should be screened for anxiety depression and those with higher depression score should undergo further evaluation. Risk factor for anxiety and depression should be assessed thoroughly and institute proper management.
Keywords: Anxiety, Depression, chronic obstructive pulmonary disease,hospital anxiety depression scale
Corresponding Author: Dr. Selvi.C, Department of Respiratory Medicine, Apollo Main Hospital, Chennai
How to cite this article: Selvi.C, Prevalence of Anxiety and Depression in Stable Chronic Obstructive Pulmonary Disease Patients in a Tertiary Care Hospital, JAPT 2019:2(1):12-17
Introduction
Chronic obstructive pulmonary disease (COPD), a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive1. Exacerbations and comorbidities contribute to the overall severity in individual patients. Its prevalence is 5.0% among Indian males and approximately 3.2% among Indian females over 35 years of age2.
| Access this article online | |
| Quick Response Code: | Website: www.aptchest.com |
The etiology between COPD and depression continues to be complex and likely bidirectional. The higher rates of smoking seen in patients with depression could lead to the higher prevalence rate of COPD in depressed patients4. However, anxiety and depression in COPD patients are often under diagnosed and contribute to the morbidity in these patients. Increased awareness is, therefore, essential to diagnose and treat psychiatric comorbidities in such patients. This study aims to study the prevalence of anxiety and depression in stable COPD patients and to correlate the severity of COPD with anxiety and depression.
Materials and Methods
This study was conducted at the department of Respiratory medicine, Apollo Main Hospitals, Chennai-6, India. Patients presenting with a well-established diagnosis of chronic obstructive pulmonary disease according to GOLD criteria were enrolled. The present study was “A Prospective cross-sectional study” conducted from December 2016 to November 2017.
Inclusion Criteria: All patients above 40 years of age, diagnosed to have COPD by pulmonary function tests (as per GOLD guidelines 2016).
Exclusion Criteria: Those Patients who were not consenting for the study, Individual with underlying psychiatric disorder, Patient who presented with acute exacerbation, Those taking oral corticosteroids – at present are excluded from the study.
Methodology
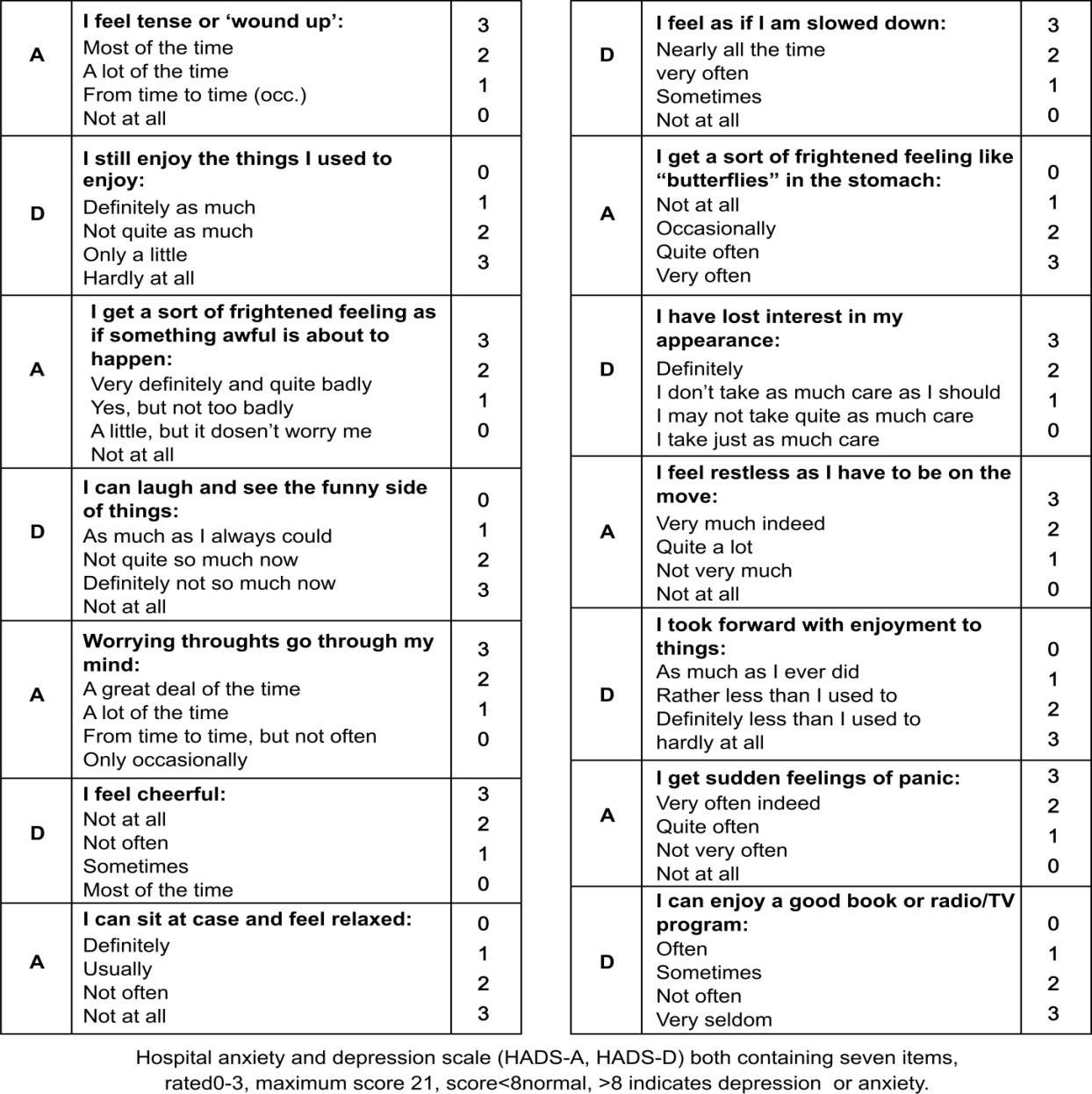
Patients present with a well-established diagnosis of COPD according to GOLD were included. In pulmonary function testing, a post-bronchodilator FEV1/FVC ratio of <0.70and COPD patients were grouped in to four severity subgroups based on airflow limitation. In patients with FEV1/FVC <0.70,GOLD 1 - mild: FEV1≥ 80% predicted, GOLD 2 - moderate: 50% ≤ FEV1 < 80% predicted, GOLD 3 - severe: 30% ≤ FEV1 < 50% predicted, GOLD 4 - very severe: FEV1 <30% predicted. Hospital scientific and ethical committee clearance was obtained before the study was started. The written informed consent was obtained from patients, or their legally acceptable representatives and they underwent a comprehensive clinical history and physical examination. Depression and anxiety were assessed by following questionnaire.
Statistical Methods
Statistical Methods: All the continuous variables will be assessed for the normality using Shapiro-Wilk test, if the variables are normally distributed; they will be expressed as Mean+SD otherwise Median (interqartile range). All categorical variables will be expressed variables, will be expressed as percentage %. Comparison of normally distributed continuous variables will be done by ‘t’ test or ANOVA based on number of groups available. Comparison of non normally distributed continuous variables will be done by MANN WHITNEY U TEST or KRUSKAL WALLIS H TEST. Comparison of categorical variables will be done by ‘Chi square Test’ or ‘Fishers exact test’ based on number of observations. Data entry will be done in Ms Excel sheet. Data analysis will be carried out by SPSS version 16.0. All ‘p’ values <0.05 will be considered as statistically significant
Results
During the study period a total of eighty patients were included in the study. Out of which sixty nine were male, 11 were female. The mean age of total study population was 59.7 ± 9.16. Total study population 80,out of which anxiety were found in39 (56.5%) males, and 2(18.2%) females, anxiety level is more in males which is statistically significant ( P value.024). Depression was found in 44 (63.8%)males and 1(9.1%) females.Depression level also more in males which is statistically significant ( P value .001). Total of 80 study population forty one (51.2%) patients have anxiety and forty five (56.3%) have depression. Thirty (37.5%) patients have both anxiety and depression. (fig1 )Total of 80 patients, 69 are smokers, out of which 40 (58%) found to have anxiety. There is a statistically significant difference in anxiety level between smoker and non smoker (P value .003).Out of 69 smokers forty four (63.8%) found to have depression. There is statistically significant difference in depression level between smoker and non smoker (P value. 001). (TABLE1), In current smokers anxiety was found in 12 (29.3%), in ex smokers anxiety was found in 28 (68.3%). There is statistically significant difference of depression among current and ex smokers P value. 002. Anxiety was found in 5 (12.2%) 20 ((48.8%) 14 (34.1%), 2 (4.9%) mild, moderate, severe, very severe obstruction respectively. Depression was found in 5 (11.1%), 21 (46.7%) 16 (36.5%) 3 (6.7%) mild, moderate, severe, very severe obstruction respectively. (TABLE2) Depression was increased significantly when disease duration increases (P value for depression. 001) anxiety also increased when disease duration increases but not statistically significant (P value. 269) (FIG2). Anxiety was found in 28 (68.3%)urban population, 13 (31.7%) rural population. Depression was found in 31(68.9%) 14(31.1%). Comorbidities found in our study population are diabetes 9 (11.25%), hypertension 30 (37.50%), coronary artery disease 9 (11.25%). There is no statistically significant association between anxiety and depression based on comorbidity.
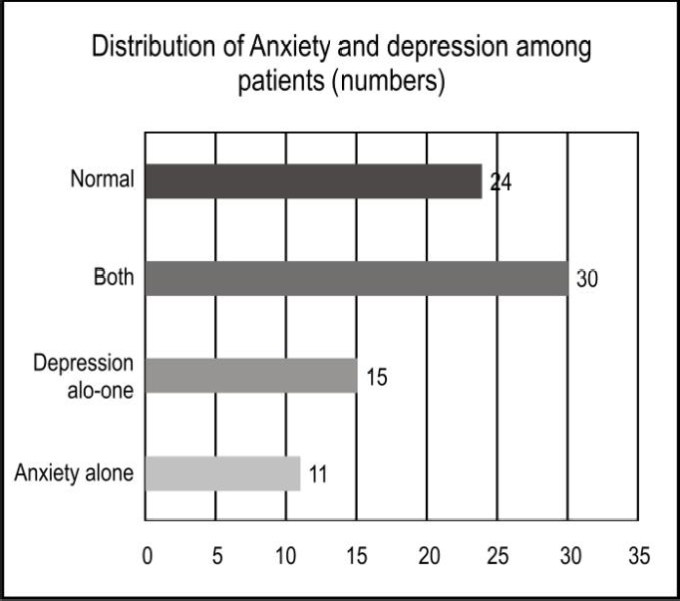
Bar diagram showing distribution of anxiety and depression among study population
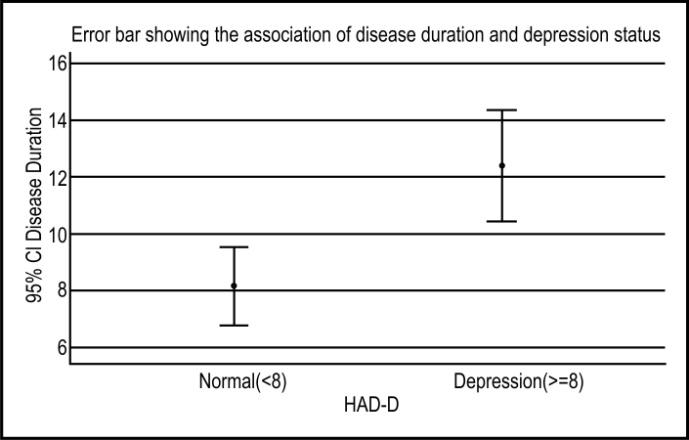
Error bar showing distribution depression in relation to disease duration
| Variables | Smoker | Non smoker | P value |
| Anxiety | 40(58%) | 1(9.1%) | .003 |
| Depression | 44(63.8%) | 1(9.1%) | .001 |
Table 1: Showing distribution of anxiety and depression among smokers and non smokers
| Variables | Mild | Moderate | Severe | Very severe | P value |
| Anxiety | 5 (12.2%) |
20 (48.8%) |
14 (34.1%) |
2 (4.9%) |
.266 |
| Depres sion |
5 (11.1%) |
21 (46.7%) |
16 (36.5%) |
3 (6.7%) |
.299 |
Table: 2 Showing anxiety and depression based on level of airway obstruction
Discussion
Our study was carried out in a Tertiary Care Hospital in India. A total of 80 patients were enrolled in the study, all of them satisfied the inclusion and exclusion criteria. Patient were divided into four groups mild, moderate, severe, very severe based on airflow obstruction. All patients were screened for anxiety and depression by hospital anxiety and depression scale (HAD A,HAD D).
Prevalence of anxiety and depression were more in patient with COPD even the disease in stable state. In our study we found anxiety was present in 51.2% and depression was present in 56.2% both anxiety and depression was found in 37.5% which is comparable to other similar study published by Kunik et al.5.In the present study 56.2% cases were depressed out of which 27.50% were having mild, 17.50% were having moderate depression and 11.25%having severe depression. Similarly out of 51.20% anxious subjects 32.50% were of mild grade 13.75% having moderate anxiety and 5% having severe depression. But severity of anxiety and depression not significantly associated with severity of COPD which is comparable with other similar study published by Wagena et al10. In our study we observed there is more anxiety and depression in moderate obstruction but there is no statistically significant association in anxiety and depression based on level of airflow obstruction in COPD which is comparable with Wagena et al. 10study.
In our study the prevalence of anxiety and depression were more in male subjects, compared to females with statistically significant difference. (P value for anxiety .024; for depression: .001), This could be due to the fact that all male subjects in our study were smokers . Anxiety and depression can be due to greater effects of smoking in males as has been shown by Wiesbeck et al6.
Kunik et al.5 and Wiesbeck et al.6 in their study they found anxiety and depression more in smoker compared to non smoker. In our study population 69 were smokers which is the major risk factor for COPD and we found 58%smokers have anxiety and 63.8% smokers have depression. There is statistically significant association between smoking and anxiety (P=.003) and depression (P=.001). In our study current smokers were 21 and ex smokers were 48 and We found ex smoker have significantly high anxiety (P=.011) and depression (.002) compared to current smokers which is comparable with Chaudhary SC et al.8 study.
More exacerbation and more disease duration associated significantly with the anxiety and depression which is observed by Chaudhary SC et al8 study Similarly in our study we found anxiety (P=.007) and depression (P=.015) significantly associated with previous exacerbation and depression (P=.001) associated significantly with disease duration.
In our study population, patients have comorbidities like hypertension, diabetes, coronary artery disease. we found that anxiety and depression not significantly associated with comorbidities this result Comparable with similar studies published by Bhowmik K et al.9
In our study we also assess the risk of anxiety and depression based on socio-economic status and we found more anxiety (43.9%) and depression (43.8%) in lower middle class but there is no statistically significant association between socioeconomic status and anxiety depression. This result can be attributed to the fact that in present study no patient were from lower class.
Kunik et al.5 found under weight patients have more anxiety and depression but in our study we found no significant association between anxiety depression and body mass index (P value .355 for anxiety,.922 for depression)this result probably due to the fact that in present study underweight patients were very less (2.5%).
In our study we also assess the risk of anxiety depression based on place of residence but we found no significant association between anxiety depression and residence (P=1) which is similar to other study published by Waseem SM et al.7
Limitations
Being a hospital-based study, finding of this study may not be generalized and it may not give the actual proportion of anxiety and depression among patients with COPD of the whole country. Recognition of comorbid depression is difficult, because some of the physical symptoms of COPD may mimic the core symptoms of depression, for example, poor sleeping pattern, anorexia and loss of enjoyment due to breathlessness which may lead to overestimation of depression among COPD patients.
Conclusion
Anxiety and Depressive symptoms are common in all stages of COPD and the prevalence of anxiety depression in Indian patients with COPD is high. Patients with COPD should be screened for anxiety depression and those with higher depression score should undergo further evaluation. Risk factor for anxiety and depression should be assessed thoroughly and institute proper management.
Recommendations
The first step to improve practice is to achieve earlier and more accurate diagnosis of these psychological comorbidities in COPD. This is important since these conditions are under diagnosed and consequently undertreated. Self-reported screening instruments are useful as an initial approach; however validated tools should then be utilized to minimize false positives and standardize care. After the psychological screening scale has been performed, high-scoring patients should be referred to a mental health specialist to facilitate access to comprehensive, gold-standard diagnosis and treatment. Due to the bidirectional nature of the association of COPD with depression and anxiety, an integrated approach that enhances the benefits between mental and physical health would be the most effective. Future studies should aim to fill the current gaps in knowledge about treatment of psychological symptoms in COPD.
Financial Support and Sponsorship
Nil
Conflicts of Interest
There are no conflicts of interest
REFERENCES
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. American journal of respiratory and critical care medicine. 2001 Apr 1;163(5):1256-76.
- Jindal SK. COPD: The unrecognized epidemic in India. The Journal of the Association of Physicians of India. 2012 Feb;60:14-6.
- Raherison C, Girodet PO. Epidemiology of COPD. European Respiratory Review. 2009 Dec 1;18(114):213-21.
- Jain A, Lolak S. Psychiatric aspects of chronic lung disease. Current psychiatry reports. 2009 Jun 1;11(3):219-25.
- Kunik ME, Roundy K, Veazey C, Souchek J, Richardson P, Wray NP, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest Journal. 2005 Apr 1;127(4):1205-11
- Wiesbeck GA, Kuhl HC, Yaldizli Ö, Wurst FM. Tobacco smoking and depression–results from the WHO/ISBRA study. Neuropsychobiology. 2008;57(1-2):26-31
- Waseem SM, Hossain M, Azmi SA, Rizvi SA, Ahmad Z, Zaidi SH. Assessment of anxiety and depression in COPD patients-A pilot study. Current Neurobiology. 2012;3(2).
- Chaudhary SC, Nanda S, Tripathi A, Sawlani KK, Gupta KK, Himanshu D, et al. Prevalence of psychiatric comorbidities in chronic obstructive pulmonary disease patients. Lung India: official organ of Indian Chest Society. 2016 Mar;33(2):174
- Bhowmik K, Adhikari A, Choudhury S, Ahmed MM. Prevalence of depression and its risk factors among patients with chronic obstructive pulmonary disease in a tertiary level hospital in West Bengal, India. South East Asia Journal of Public Health. 2013 Jul 30;2(2):34-40.
- Wagena EJ, Arrindell WA, Wouters EF, Van Schayck CP. Are patients with COPD psychologically distressed?. European Respiratory Journal. 2005 Aug 1;26(2):242-8




