
689 views
Monisha Anandhan et al.: Pulmonary Agenesis – A Zebra Like Disorder for Pulmonologists
Pictorial CME
Pulmonary Agenesis – A Zebra Like Disorder for Pulmonologists
Monisha Anandhan1, Amal Johnson2 and Narasimhan.R3
1 Post graduate, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai, India
2 Post graduate, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai, India
3 Senior Consultant, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai, India
ABSTRACT
Pulmonary agenesis is an extremely rare congenital anomaly defined as a complete absence of the lung parenchyma, bronchus, and pulmonary vessels. In case of complete unilateral agenesis, no pleural cavity can be found on the affected side. More than 50% of children with lung aplasia die within five years of birth but some individuals live a normal life span with their deformity and may be asymptomatic throughout life. Respiratory tract infections are the greatest danger in these individuals. We report a case of left lung aplasia with bronchiectasis in a young aged adult who was treated for tuberculosis and was referred to our institute for persistent cough.
Keywords: Lung agenesis, aplasia, hypoplasia
Corresponding Author: Dr. Monisha Anandhan, Post graduate, Department of Respiratory Medicine, Apollo Hospitals, Greams Road, Chennai, India
How to cite this article:Monisha Anandhan, Amal Johnson, and Narasimhan.R, Pulmonary Agenesis – A Zebra Like Disorder for Pulmonologists, JAPT 2018; 2:83-86
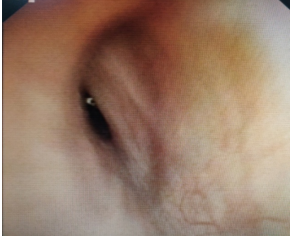
Left rudimentary bronchus
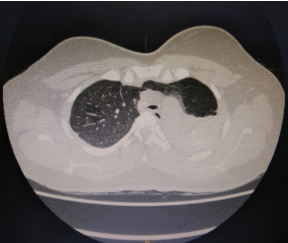
Total absence of left lung and increase volume of right lung.
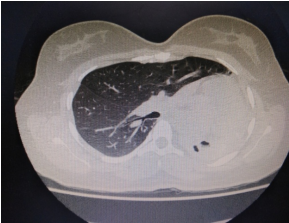
Ipsilateral shift of the mediastinum

Main carina – Left rudimentary bronchus is present
Introduction
Pulmonary agenesis is defined as complete absence of bronchus, parenchyma and vessels. The lung first appear as an epithelial bud or pouch from primitive foregut (endoderm) at the caudal end of the laryngeotracheal groove in the 3rd week of gestation. This deepens and the constricts, there by forming a separate ventral trachea and a dorsal oesophagus. The ventral trachea elongates and bifurcates to form two separate bronchial lung buds. These primary bronchi continue to grow into the splanchnic mesenchyma. Lung development is subdivided into three main period the embryonic period, the fetal period and postnatal lung development. Lung organogenesis is part of the embryonal period. While fetal lung development consists in the pseudoglandular, canalicular and saccular stages, postnatal lung development comprises the stages of classical and continued alveolarization, as well as of microvascular maturation. Vascular endothelial growth factor (VEGF) plays important role in lung development. Other factors sonic hedgehog (SHH) and Fibroblast growth factor(FGF). The failure of bronchial analogue to divide equally between two lungs with possible abnormal blood flow in dorsal aortic arch during this period may result in hypoplasia, aplasia and agenesis of unilateral pulmonary parenchyma. For diagnosis of pulmonary agenesis different imaging techniques can be used. Plain chest shows unilateral opaque lung with mediastinal shift whereas for final diagnosis CT scan, MRI bronchography, bronchoscopy and pulmonary angiography are used. Sometimes the disease can be detected in prenatal life by the help of prenatal ultrasound showing hyperechoic hemithorax however the definitive diagnosis is hard which can be confirmed by Fetal MRI.
Case Reports
A 24 year old lady presented as an outpatient with the complaints of cough for 4 year, with the increased severity over last 6 months. She had non productive cough for 6 months. There was no history of fever, hemoptysis, chest pain, wheeze and breathlessness. She reported occurrence of such episodes of cough in the past since her childhood for which she had taken over the counter medication multiple times. She also gave history of being treated for tuberculosis 5 years back by a private practitioner. She completed the antituberculous treatment for 6 months. As her symptoms kept on worsening, she was referred to our institute for further evaluation. On examination she was afebrile. Her respiratory rate was 18 per minute; her SpO2 was 96% at room air. There was reduced respiratory movement over the left mammary region. On palpation, expansion was reduced over the left hemithorax. The trachea was shifted to the left side and on auscultation; air entry was decreased over the left side of the chest. On the right side, there were vesicular breath sounds. Her chest X-ray showed a homogeneous opacity in the middle and lower zones on the left side with marked shift of the mediastinum to the left. CT chest with contrast with 320 slice revealed total absence of left lung with herniation of right lung and increase volume of right lung. Mediastinal structures including heart and great vessels were displaced to middle and lower parts of left hemithorax. Left pulmonary artery was absent. Left main bronchus was rudimentary.
Discussion
Pulmonary underdevelopment has been classified into three groups by Schneider and Schwalbe. Group 1 (Agenesis): Complete absence of bronchus, lung and pulmonary vasculature; Group 2 (Aplasia): Rudimentary bronchus is present but lung parenchyma and vessels are absent; Group 3 (Hypoplasia): Reduction in the number or size of airways, vessels and alveoli. In our case, patient had Type 1 left lung aplasiawithout any other anomaly and hence, had a better prognosis.
Pulmonary Agenesis and Aplasia
It occurs on either side. Radiographically, it results in
- Opacification of a affected hemithorax
- The markedly reduced volume results in elevation of the ipsilateral hemidiaphragm, ipsilateral shift of the mediastinum (The heart is displaced into the posterior hemithorax on the side of agenesis or apalsia, along with other medistinal structures) and approximation of the ribs.
- On lateral radiographs, the anterior chest appears abnormally lucent because of herniation of the remaining lung into the opposite hemithorax
- In patients with apalsia, CT can demonstrate the rudimentary bronchus, as well as absence of the ipsilateral pulmonary artery. In patients with agenesis, bronchi are also absent.
- In most of the cases, the contralateral lung is greatly overinflated and displaced.
Pulmonary Hypoplasia
Pulmonary hypoplasia represents abnormal lung development associated with a reduction in lung volume and often a decrease in the number of alveoli and bronchial divisions. There may also be anomalous lobes or segments, or they may be reduced in number. Narrowing between the ribs and elevated hemidiaphragm on this side is also observed. CT can demonstrate
- The patent bronchus
- The pulmonary artery
- The hypoplastic lung
Differential Diagnosis
Pneumonectomy performed during early childhood. The radiological findings may be identical.
Total atelectasis from any other cause
- Severe bronchiectasis with collapse
- Advanced fibrothorax.
- The main differential diagnosis of hypoplastic lung is Sweyer-JamesMCLeod syndrome. Although both conditions are associated with unilateral low lung volume, patients with SweyerJames-MCLeod syndrome demonstrate air trapping on radiographs or CT scans performed at the end of maximal expirations.
Conclusions
Bronchopulmonary anomalies in adults are usually asymptomatic. Symptoms may be due to superimposed infection or compression of an adjacent airway, vessels or lungs. Congenital anomalies of the chest are an important cause of morbidity in infants, children, and even adults. The evaluation of affected patients frequently requires multiple imaging modalities to diagnose the anomaly and plan surgical correction.
Acknowledgement
We sincerely thank the management of Apollo Hospitals for their consistent support in our pursuit for excellence.
References
- Adel El-Badrawy and Mohammad K. El-Badrawy, Adult presentation of asymptomatic right lung agenesis: a rare anatomical variation, Surgical and Radiologic Anatomy, 10.1007/s00276-018-2130-1, (2018).
- Nguyen KM, Vala S, Milla SS, Guglani L (2018) Unilateral lung agenesis, aplasia or hypoplasia: which one is it? Congenit Anom (Kyoto) 58(2):75–76.
- Wu CT, Chen MR, Shih SL, Huang FY, Hou SH. Case report: Agenesis of the right lung diagnosed by three dimensional reconstruction of helical chest CT. Br J Radiol. 1996;69:10524.
- NCCP textbook of Respiratory medicine.
- Muller silva Imaging of the chest.
- Congenital Anomalies of the Tracheobronchial Tree, Lung, and Mediastinum: Embryology, Radiology, and Pathology Teresa Berrocal, Carmen Madrid, Susana Novo, Julia Gutiérrez, Antonia Arjonilla, Nieves Gómez-León
- The Embryology of the Lung Lynne Reid.
- Computed tomographic estimation of lung dimensions throughout the growth period
- P. A. de Jong, F. R. Long, J. C. Wong, P. J. Merkus, H. A. Tiddens, J. C. Hogg, H. O. Coxson
- European Respiratory Journal 2006 27: 261-267.




