
694 views
Bilateral Catamenial pneumothorax with Catamenial Hemoptysis
Bilateral Catamenial pneumothorax with Catamenial Hemoptysis
Selvi C, Govindasamy C, Narasimhan.R
Department of Respiratory Medicine, Apollo Hospitals, Chennai, Tamilnadu, India
Abstract
Bilateral catamenial pneumothorax coexisted with catamenial hemoptysis is a rare entity. It is usually caused by thoracic endometriosis syndrome. We report a case 24 year healthy female with no comorbid status presenting with bilateral catamenial pneumothorax with catamenial hemoptysis. This lady presented with breathlessness, bilateral chest pain and streaky hemoptysis for four months associated with her menstrual cycle. Chest x ray and CT chest done showed bilateral pneumothorax. Serum CA 125 levels was elevated.USG pelvis done was normal. Bronchoscopy was done in view of hemoptysis showed bilateral inflamed mucosa no active bleeding. Videothoracoscopy was done showed multiple nodules over the diaphragm, biopsy taken from that nodules following biopsy, diaphragmatic meshplasty and talc pleurodesis was done. To prevent the recurrence patient was started on hormonal therapy. Patient improved clinically and radiologically and no recurrence till one year of followup.
Keywords: Breathlessness, Hemoptysis, Pneumothorax, Videothoracoscopy, Meshplasty ,Pleurodesis
Corresponding Author: Dr.Narasimhan.R, Department of Respiratory Medicine, Apollo Main Hospitals, 21, Greams Lane, Off Greams Road, Chennai – 600 006, Tamil Nadu, India.
How to cite this article: Selvi C, Govindasamy C, Narasimhan.R, Bilateral Catamenial pneumothorax with Catamenial Hemoptysis, JAPT 2019: 2(2):68-71
Introduction
Catamenial pneumothorax (CP) is a recurrent spontaneous pneumothorax occurring in women associated with a period of menstruation. Catamenial pneumothorax occurs due to the presence of ectopic endometrial tissue in thoracic cavity.1,2. Endometriosis of thoracic cavity is a rare entity; it consists of four clinical types: Catamenial pneumothorax, Catamenial hemothorax, hemoptysis and pulmonary nodules 3,4. CP usually occurs within 24 hours before and 72 hours after the onset of menses and appears almost exclusively in the right hemithorax1. Around 60% of thoracic endometriosis cases are associated with pelvic endometriosis1,5. Cause for thoracic endometriosis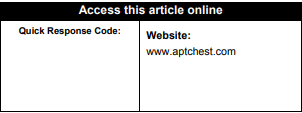
is not clear but most acceptable theory explains the retrograde implantation of endometrial tissue by lymphatic and haematogenous dissemination or presence of diaphragmatic defects 2. Upto 85 to 90% of cases of CP usually occurring on right side. A combined surgical and hormonal treatment is the management of choice for CP. Hormonal therapy prevent the postoperative recurrences.3,6. We report a catamenial pneumothorax occurring bilaterally along with catamenial hemoptysis which was successfully treated with combined surgical and hormonal therapy.
Case Report
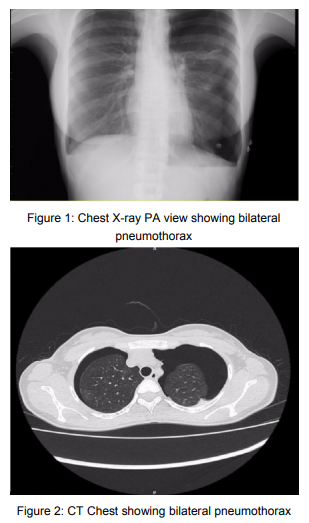
24 year old healthy woman presented with symptoms of breathlessness and chest pain and hemoptysis for past 4 months associated with her menses. First three episode resolved spontaneously. This time she had increasing breathlessness, chest pain and hemoptysis. On presentation patient was tachypneic her respiratory rate was high, other vitals stable. On respiratory examination Bilateral decreased chest movements and decreased breath sounds was heard. Her hematological and biochemical parameters were normal. HIV serology was negative. Her CA125 level was elevated(56U/ml). Chest X-ray was done showed bilateral pneumothorax (Fig. 1). Computed tomography (CT) done showed bilateral pneumothorax (Fig. 2). Ultrasonography of pelvis excluded the presence of pelvic endometriosis
Hypothesis of catamenial pneumothorax and catamenial hemoptysis was taken into account .the patient underwent a bronchoscopy showed inflamed mucosa on both side, no active bleeding.
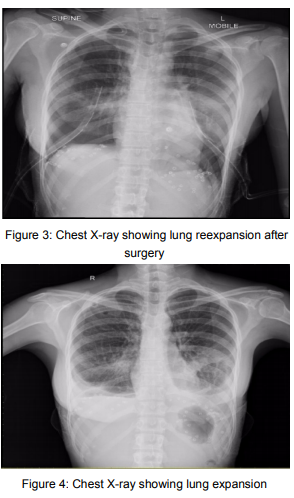
videothoracoscopic exploration of the bilateral pleural cavity under general anesthesia was done, first in right lateral position by two ports approach pleural cavity explored, multiple purple red nodules were seen in the diaphragm. Biopsy taken from that nodules .Patient repositioned and redraped and procedure repeated on right side, Talc pleurodesis done bilaterally followed by bilateral meshplasty of diaphragm done. After control of hemostasis a ICD drain was placed in pleural space and full lung re-expansion achieved (Fig. 3). The chest tube was removed after 2 days of surgery (Fig. 4).
Final pathology confirmed endometriosisrelated catamenial pneumothorax (ER–CP) according the most updated classification by Legras et al.8. After surgery the patient was started hormonal therapy with 17 etinil testosterone 800mg daily then shifted to dienogest 2mg daily. No recurrence has been observed till 3 months post surgery
3. Discussion
We report a rare case of bilateral Catamenial pneumothorax (CP) coexisted with catamenial hemoptysis. It is a rare entity characterized by lung collapse during menstruation due to thoracic endometriosis. CP most commonly occurs in 30 -50 years of premenopausal women with history of infertility.
Thoracic endometriosis syndrome consists of two types. Pulmonary form and pleural form. Pulmonary form manifests as catamenial hemoptysis and pulmonary nodules. Pleural endometriosis manifests as catamenial pneumothorax, catamenial hemothorax, catamenial pneumomediastinum and chest pain11. Several pathogenic mechanisms have been evoked CP. The metastatic theory presume the transdiaphragmatic passage of endometrial tissue by lymphohematogenous dissemination or congenital fenestration. The anatomical theory explains for dissolution of cervical mucus plug during the menses with migration of cells through vagina, uterus, fallopian tubes to peritoneum and air reaching the chest by diaphragmatic congenital fenestrations. In the hormonal theory prostaglandin F2 mediated pulmonary vasospasm during ovulation leads to ischemic injury and alveolar rupture4,6. Congenital diaphragmatic defects are more common on the right side and also more lymphatic drainage and clockwise peritoneal circulation that sweeps endometrial implants to right side this explains CP most commonly occur on right side11,12.
The diaphragmatic defect(s) can be single or multiple, commonly occur at the central tendon, this defects may be tiny holes (1–3 mm), or larger defects (>10mm)13. High resolution computed tomography (HRCT) to detect endometrial deposits in the lung and pleura. USG of pelvis to detect pelvic endometriosis because around 50 to80% pulmonary endometriosis associated with pelvic endometriosis.14,15. Both thoracic and pelvic MRI are considered superior to CT due to the blood products in the endometrial deposits11,16.
CA125 (Cancer Antigen 125) is a tumor marker used for monitoring treatment and detecting recurrence of ovarian cancer. It also elevated in benign ovarian conditions also. Endometriosis also been associated with increased levels of CA-125, and although it is not considered a specific marker, it can assist in early diagnosis of endometriosis-related pneumothorax 13,17.
Bagan et al conclude that this CA-125 biological marker may favor indication of videothoracoscopy and hormonal therapy at an early stage in the prevention of catamenial pneumothorax recurrences, and should be evaluated prospectively in a larger-scale studx 18.
Cyclical haemoptysis at the time of menstruation is called catamenial hemoptysis. Diagnosis by detection of endometriotic plaques on bronchial washings and endometrial tissue on lung biopsy. However, these may be negative despite the presence of the disease. Computed tomography scan of the chest during the days of menstruation and in midcycle shows ‘ground-glass’ or patchyinfiltrate appearance during the menstrual days and clear lung fields in midcycle.
Management of Thoracic endometriosis can be medical or surgical. Medical treatment using 17etinil testosterone or danazol it suppresses the production of gonadotropins, endometrial hypotrophy thus leading to a condition of pseudomenopause and finally a remission of the disease.14,20. Endometriosis is a hormone dependent disease so when medical therapy stopped disease will get recur morethan 50%within 6 months of treatment.20. The surgical treatment combined with hormonal therapy is recommended modality of treatment4,21.
Surgical treatment should be done during menstruation for better visualization of pleurodiaphragmatic endometriosis. Videothoracoscopy is a very useful tool since it assesses both the diaphragmatic surface and the pleural cavity and is able to detect multiple nodules although it has been reported, No pathologic findings were reported in 8.5%cases1,3. Suturing the defect, endoscopic resection of the area, covering the diaphragmatic surface with polyglactin mesh are the common surgical procedures but which do not completely prevent the risk of CP to recur. Pleurodesis plays a major role when microscopic endometrial foci or newly implanted lesions cannot be detected2,12. In our case we found multiple nodules in posterior diaphragmatic surface but fenestrations were detected. we preferred our surgical procedure to biopsy from the lesion and diaphragmatic meshplasty and talc pleurodesis, and combine it with the hormonal treatment to achieve the best outcome.
4. Conclusion
Coexisting bilateral Catamenial pneumothorax and catamenial hemoptysis is a rare presentation. So videothoracoscopy provides magnification and better visualization of the pleural cavity and diaphragm. Among surgical options videothoracoscopic resection of detected lesions combined with pleurodesis with diaphragmatic meshplasty is the most successful one and, associated with hormonal therapy, reduces the risk of recurrence.
References
1. A.N. Visouli, K. Darwiche, A. Mpakas, et al., Catamenial pneumothorax: a rare entity? Report of 5 cases and review of the literature, J. Thorac. Dis. 4 (S1)(2012) 17–31.
2. C. Nezhat, J. Main, C. Paka, A. Nezhat, R.E. Beygui, Multidisciplinary treatment for thoracic and abdominopelvic endometriosis, JSLS 18 (2014) 1–7.
3. S. Attaran, A. Bille, W. Karenovics, L. Lang-Lazdunski, Videothoracoscopic repair of diaphragm and pleurectomy/abrasion in patients with catamenial pneumothorax. A 9-year experience, Chest 143 (2013) 1066– 1069.
4. P. Azizad-Pinto, D. Clarke, Thoracic endometriosis syndrome: case report and review of the literature, Perm. J. 18 (2014 Summer) 61–65.
5. A. Veeraswamy, M. Lewis, A. Mann, S. Kotikala, B. Hajhosseim, C. Nazhat, Extragenital endometriosis, Clin. Obstet. Gynecol. 53 (2010) 449–466.
6. D. Papafragaki, L. Concannon, Catamenial pneumothorax: a case report and review of the literature, J. Women’s Health 17 (2008) 367–372.
7. P. Ciriaco, G. Negri, L. Libretti, et al., Surgical treatment of catamenial pneumothorax: a single centre experience, Interact. Cardiovasc. Thorac. Surg. 8 (2009) 349–352.
8. A. Legras, A. Mansuet-Lupo, C. Rousset-Jablonski, A. Bobbio, P. Magdeleinat, N. Roche, J.F. Regnard, A. Gompel, D. Damotte, M. Alifano, Pneumothorax in women of childbearing age: an update classification based on clinical and pathologic findings, Chest 145 (2014) 354–360.
9. P. Athwal, K. Patel, C. Hassani, S. Bahadori, P. Nardi, A case of multisystem endometriosis, J. Radiol. Case Rep. 7 (2013) 1–6.
10. C. Rousset-Jablonski, M. Alifano, G. Plu-Bureau, et al., Catamenial pneumothorax and endometriosis-related pneumothorax: clinical features and risk factors, Hum. Reprod. 26 (2011) 2322–2329.
11. P.S. Chatra, Thoracic endometriosis: a case report, J. Radiol. Case Rep. 6 (2012) 25–30.
12. V. Baysungur, C. Tezel, E. Okur, B. Yilmaz, Recurrent pneumothorax diagnosed as catamenial after videothoracoscopic examination of the pleural cavity, Surg. Laparosc. Endosc. Percutan. Tech. 21 (2011) 81–83.
13. A.N. Visouli, K. Zarogoulidis, I. Kougioumtzi, et al., Catamenial pneumothorax, J. Thorac. Dis. 6 (S4) (2014) 448– 460.
14. S.Z.A. Badawy, P. Shrestha, Recurrent catamenial pneumothorax suggestive of pleural endometriosis, Case Rep. Obst. Gynecol. (2014) 1–2, http://dx.doi.org/10.1155/2014/756040.
15. D. Soriano, R. Schonman, I. Gat, E. Schiff, D.S. Seidman, H. Carp, A.Y. Weintraub, A. Ben-Nun, M. Goldenberg, Thoracic endometriosis syndrome is strongly associated with severe pelvic endometriosis and infertility, J. Minim. Invasive. Gynecol. 19 (2012) 742–748.
16. P. Rousset, C. Rousset-Jablonski, M. Alifano, A. MansuetLupo, J.N. Buy, M.P. Revel, Thoracic endometriosis syndrome: CT and MRI features, Clin. Radiol. 69 (2014) 323–330.
17. P. Santulli, I. Streuli, I. Melonio, L. Marcellin, M. M’Baye, A. Bititi, B. Borghese, M.C. for severity of deep endometriosis, J. Minim. Invasive. Gynecol. 22 (2015) 275– 284.
18. P. Bagan, P. Berna, J. Assouad, M. Riquet, et al., Value of cancer antigen 125 for diagnosis of pleural endometriosis in females with recurrent pneumothorax, Eur. Respir. J. 31 (2008) 140–142.
19. P.J. Pickhardt, M.E. Hanson, Incidental adnexal masses detected at low-dose unenhanced CT in asymptomatic women age 50 and older: implications for clinical management and ovarian cancer screening, Radiology 257 (2010) 144–150




